



In 2018, Public Health England listed ‘novel coronavirus’ as a CBRN ‘biological threat’…
Was this the template for death-by-neglect of vulnerable people in locked-down facilities during the COVID operation?

Since December, this substack has focused on the evidence pointing to ‘CBRN incident response’ as the framework for the international lockstep operation - most noticeably seen in the Five Eyes countries - from mid-March 2020 onwards.
Previous posts have looked at documents from the US and also Australia.
This post looks at a ‘front-line’ CBRN document published by Public Health England in 2018 which has direct relevance to the COVID event.

Post-publication update on 7 February 2025: Please read this timely breaking news from
on the UK COVID-19 inquiry and what he describes as…“The normalisation of the abnormal. Medical totalitarianism.”
WHEN the next pandemic comes having a test trace and isolation system in place…so it can be quickly put into operation will be vital to our pandemic response.

Public Health England 2018 Chem-Bio-Rad-Nuc Incident Handbook
10 points at a glance
1. In 2018, Public Health England published a 148 page document on clinical management of CBRN (chemical, biological, radiological and nuclear) incidents…
“The audience for this publication remains to be first responders, emergency departments and public health and health protection professionals.” (p7)

Biological agents: Deliberate release incidents (p68)
This manual focuses on organisms that could be aerosolised and/or would cause serious or fatal infections.
(Sounds serious! Recall that leading experts said COVID was “… a low risk infection… even in the absence of a vaccine.”)
2. Section on “Think of coronavirus infections” states:
(p 90)
Any patient who meets this definition has a novel coronavirus/SARS/MERS until proven otherwise: fever more than 38 C and cough or dyspnoea or breathing difficulty and in the ten days before onset of illness….
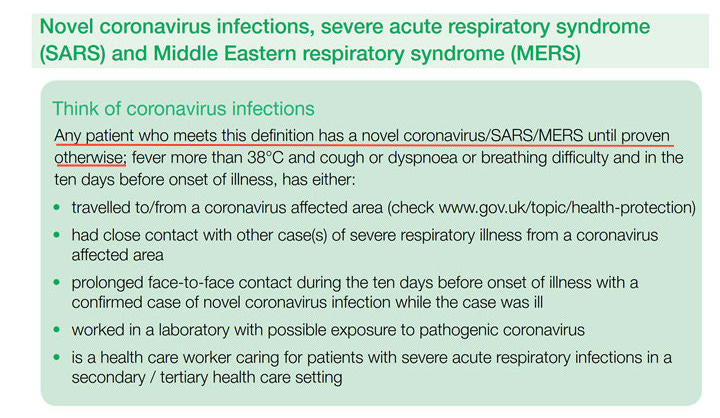
(Crikey… a lot of latitude here. Until ‘proven’ by the PCR test!)
3. The term “novel coronavirus” is used several times in the document and the following “key fact” is prominently presented:
Human coronaviruses do not currently occur naturally in the UK.
(What about the common cold? Are they telling us these pathogens occur unnaturally?)
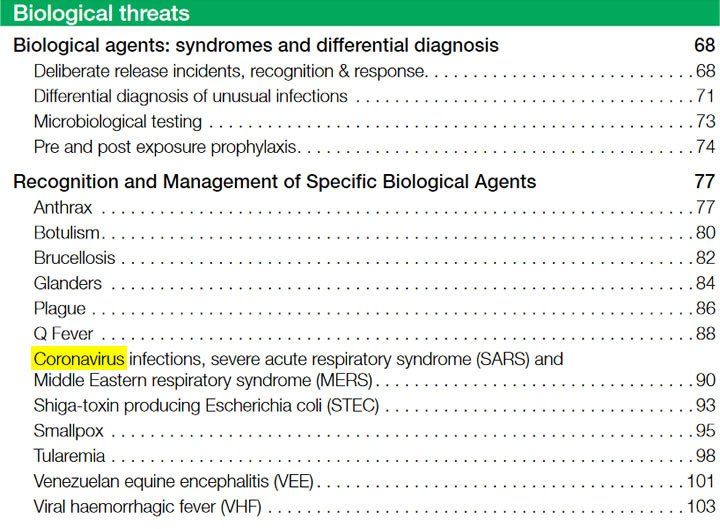
4. A list of ‘specific biological agents’ includes coronavirus infections
Coronavirus infections - highlighted below in yellow (p5).
(Note: Influenza is not on the list of ‘biological agents’ despite longstanding hype about “influenza as a bioweapon” in the two decades before the COVID event.)
5. “Differential diagnosis of unusual infections”
In another diagram, the common symptoms and signs of coronavirus are shown in common with many other conditions (p71):
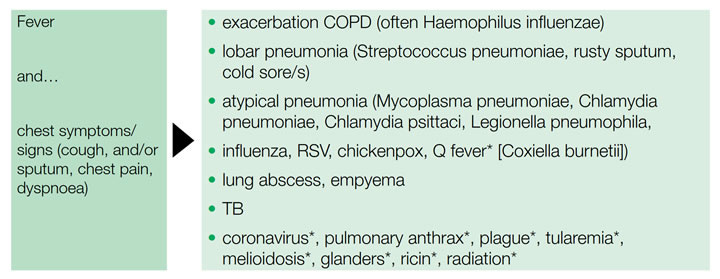
(So unusual infections look a lot like common infections?)
6. A need for “rapid detection and early isolation of [coronavirus] cases” is emphasized:
Management of suspected cases of coronavirus includes (p91):
If patient satisfies case definition, and condition warrants, admit to single isolation (ideally negative pressure) room, with airborne infection isolation precautions including P3 respirator.
(This sounds like the management of Ebola - aka “Viral haemorrhagic fever” - per p104)
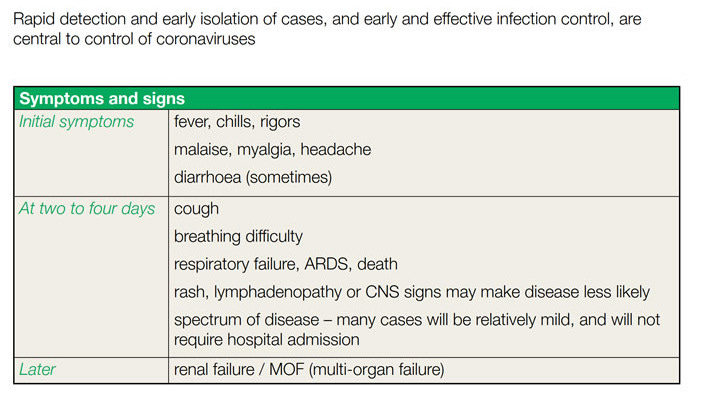
7. There is also conflicting advice as to the recommended ‘Ebola'-level isolation of coronavirus cases:
spectrum of disease - many cases will be relatively mild and will not require hospital admission
(So… not serious or fatal in most cases. Hence the need for asymptomatic super-spreaders.)
8. A section on Personal Protective Equipment (PPE) includes a flow chart for CBRN incidents
(partial screen shot below - p13)
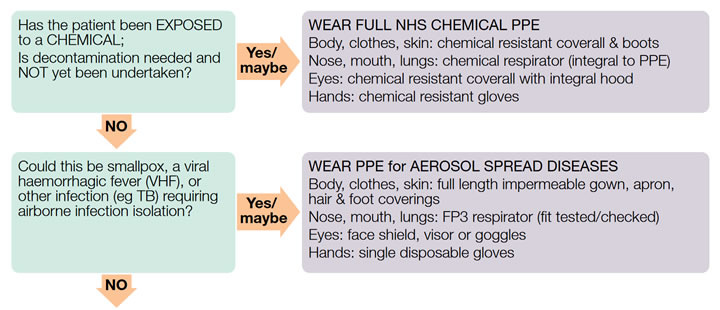
The full chart indicates precautions as for ‘Aerosol Spread Diseases’:
If coronavirus suspected - FP3 respirator (fit tested/checked)
(And other Ebola-level precautions for suspected coronavirus!)
9. “Biological Threats: Recognition of release incidents”
There are two noteworthy points that are relevant to the COVID event in terms of both the official narrative (and counter-narrative) and the potential reality (p68):
Intentional and naturally occurring outbreaks may be indistinguishable initially
Symptoms of some forms of intentional or accidental chemical poisoning may mimic some infections
(Interesting!)
10. The document mentions High Consequence Infectious Diseases (HCID)
This is directly relevant to the COVID event because Public Health England downgraded COVID-19 from a suspected HCID on 19 March 2020 - applicable in England, Wales, Scotland and Northern Ireland - based on “low overall mortality rates”.
As of 19 March 2020, COVID-19 is no longer considered to be a HCID in the UK.
(So… only a low-risk ‘pandemic’, then. No need to lockdown and mask and force-vaccinate entire populations.)

The 2018 Public Health England handbook on ‘CBRN incidents’ which outlines the clinical management of “novel coronavirus” raises many questions, including…
Was this prescient document - full of fear-mongering and misinformation - the origin of the inhumane “infection control” practices imposed on captive inpatients and residents in “healthcare” and “aged care” and “disability care” facilities during the COVID lockdowns… measures which directly led to the deaths-by-neglect of vulnerable people due to denial of their most basic needs?

For further harrowing details of the COVID charnel houses, see coverage of the Scottish and UK COVID inquiries by
…There are many more questions to be asked…
Not only within the UK, but in every nation where pre-planned Ebola-level physical isolation together with the deliberately-induced panic over “inadequate PPE” was rolled out as a lethal weapon to create the illusion of deaths ‘due to the pandemic’.
Postscript:
See this post for more on the the Axis of Anglos during COVID:

Also…. many thanks to independent researcher at for her invaluable input and assistance.
Please see the following posts by Elizabeth, including articles with a specific UK-focus.

Elizabeth Evans, CEO of the UK Medical Freedom Alliance
A doctor explains informed consent for vaccination...
Rupert Lowe, Reform UK MP